It's apparently sourced, but first match only finds usage in this Feb 2016 slideshow: http://www.slideshare.net/athenahealth/thriving-as-an-independent-practice
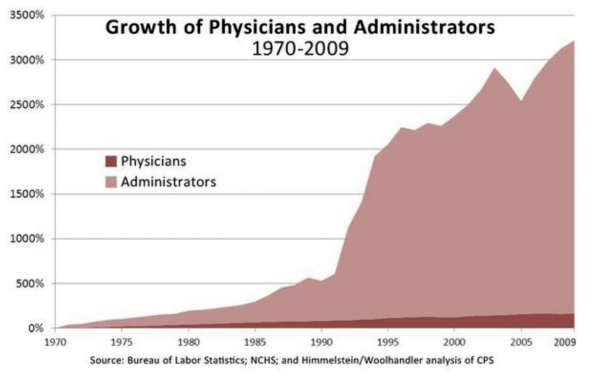
I can't make sense of it. The vertical axis is a percent, but what scales 100%? It starts with near 0% in 1970. If you look at the 100%, the administrators cross that around 1975, while the doctors cross 100% around 1995. So what could that mean!?
Here's another one, with doctors, nurses, and administators in slide 60, and something similar 1970-1998, starting near zero, and rising over 2000. http://www.slideshare.net/bayarea/healthcare-presentation-iafpe-sep-12-2009
Okay, so maybe 0% is what I'd call 100%, and 100% is a doubling. So the number of administrators in 1998 is 20 times as many as 1970, while doctors slightly more the doubled, 1.3 times more. And nurses rose more than doctors, which at least makes sense, shifting care tasks to lower skilled workers.
I wouldn't suppose people like lab technicians would be "Administrators", but it makes sense with more diagnostic technology there'd be more non-doctors doing work that didn't exist in 1970. But I'd not assume that meaning.
One more chance on source statement... Bureau of labor statistics; NCHS; and Hammelstein/Woolhandler analysis of CPS Growth of Administrators 1970-2009
Who are Hammelstein/Woolhandler?
Ah, pro-single payer! So now I wonder if they're also including the insurance industry?
http://www.bostonglobe.com/opinion/2012/06/01/single-payer-health-care-would-save-billions-for-massachusetts/yNTLRlKucgdJCUCU3P5arM/story.html ------- Here are six alternative steps the Legislature could take that would actually save money while still preserving care.
■ Cut out the middlemen. Why exactly do we pay private insurers 10 cents of every premium dollar? The plan that covers all 13 million residents of the Canadian province of Ontario has overhead of only 1 percent. Adopting that single-payer approach in Massachusetts would save about $2 billion in insurance overhead in 2013 alone.
■ Pay hospitals the way we pay fire departments: real global budgets that cover all operating costs, not the per-patient schemes that are masquerading as global payments. Billing, collections, and paperwork consume nearly one quarter of hospitals’ revenues. Eliminate billing for individual patients and you’d cut that nearly in half. The savings: about $3 billion in 2013.
■ End the medical arms race and enforce real health planning. ■ Right-size the physician work force: more primary care, fewer specialists.
■ Negotiate drug prices statewide. Canadians pay 40 percent less for drugs than we do because they use single-payer buying power to drive down prices from pharmaceutical companies. Why can’t we?
■ Cap health executives’ incomes. Why should a hospital CEO make more than the president of the United States?
David U. Himmelstein, M.D. and Steffie Woolhandler, M.D., M.P.H. co-founded Physicians for a National Health Program. They are professors at the City University School of New York School Public Health and visiting professors at Harvard Medical School. They worked as primary care doctors in Massachusetts from 1982-2010. ------
Ares, if you believe single-payer healthcare works, you'll believe in leprechauns, fairies and yetis, too. Just give me one example where central planning works in the long run. No one person, organization or entity is capable of running 1/7th of the American economy, or much else. None of those six alternative steps will work.
My favorite part is: "Negotiate drug prices statewide." So we'll have 51 different states negotiating drug prices, eh? Well, if 51 is great, why not one? That's what single-payer is: ONE single payer. Canadians pay 40% less for drugs because they're free riders on pharmaceutical innovation. Unless medical innovation isn't important to you, and you're willing to submit to rationed care at the discretion of some nameless, faceless, unaccountable bureaucrat. You probably believe you can have "Better care, at a lower cost." Just like "If you like your doctor, you can keep your doctor."
And please enlighten me about why the President of the United States' annual salary has anything to do with a hospital CEOs compensation package? Do you understand anything about compensation structures?
The government knows all, sees all, and can produce any outcome. That's magical thinking. Central planning never works in the long run... it never lives up to its promises. Quality descends and costs skyrocket. For anything it touches. When will you people ever understand the human condition, and that government is run by human beings? Why would you ever want to centralize human flaws into one source? What is it that scares you so much about distributed sources? I thought we were supposed to "celebrate diversity." The government kills diversity.
Then again, you believe in anthropomorphic climate change. How do you like the states attorneys general going after private companies and think tanks for their dissent? Celebrate diversity, indeed! We'll have all kinds of diversity... just not the thought kind!
The Left claims to be the vanguard of some euphoric free-for-all xanadu society. What we end up with is the misery of totalitarianism.
Anonymous at 2:36 PM said... When you have no argument, you attack the data.
Who is attacking and what data?
My small accomplishment was to discover the source the graph was by two doctors supporting single-payer for Massachusetts.
I'm not sure what IAC is ranting about, although lots of bitterness there.
On the 51 plans, Minnesota is also looking at single-payer plans, and once individual states show that works, it makes sense other states won't bother reinventing the wheel. Perhaps it will end up as regional things with groups of like-minded states working together.
Soon I guess Minnesota and Company can also be "free riders on pharmaceutical innovation." It'll be a good deal for us.
Who knows, maybe there are better business plans than "invent a drug, make up a illness that it helps, suppress the side-effects, give free samples to doctors, and complain that the 10,000% markups are just market economics in play."
Anyway, life will be better when some of that "administration" bloat that Stuart discovered is reduced. Or at least maybe we can figure out who they are and what they're doing before we make their jobs obsolete.
I guess I'm a bitter clinger, Ares. I'm bitter about people believing self-evident economic stupidity and I am clinging to as much of a private healthcare system as possible.
Perhaps you could at least consider -- if just for a moment -- that the increase in administration is because there's more to administrate. What's driving the need for so much administration? Did you ever once consider that? What they're doing is keeping government, insurance companies and lawyers at bay... just like education. Government workers, trial lawyers and teachers unions are significant Democrat donor constituencies. How is it you can be so cynical about the private sector's motives and ignore the public sector's motives? Do you really think government will make things FREE?
Democrats celebrate diversity and are pro-choice... unless it's economic diversity or economic choice.
Your level of ignorance is breathtaking. Government will solve all our problems! Enjoy your single-payer plan in Minnesota.
IAC, for some reason public funded roads are okay for you, but public funded health care is not. Do we think roads are free? No, we pay taxes for them, and the rich pay a larger share.
As long as we require hospitals to treat everyone with emergency care, you can be sure some people are not going to have insurance, and not go in until they need emergency care and can't be refused. And hospitals pass on those costs to everyone else.
And if you don't have insurance, and plan to pay with cash you'll face "charge masters" rates that are jacked up many times higher than anyone actually pays who has insurance, because insurance companies can refuse to pay more than some amount, and different insurance companies have different rates they'll pay, so hospital "charge master" rates exist to maximize returns from all the permutations of insurance companies polices in an endless evolutionary war of attrition.
And if you're Ron Paul with $100,000 in your savings account, and no insurance, good luck trying to negotiate which hospital emergency room will give you the best price on your surgery after your car accident. You can refuse to pay of course, and then see your credit score plummet, which actually might not be a bad thing if you have $100k in the bank and no need for credit. I'm not sure all the things debt collectors can do to you, but I'm sure they can make your life miserable if you owe enough.




10 comments:
Curious.
Matches the growth in education administration, I'm sure.
Wharton earth might they be administrating?
Keep in mind: The only two industries whose costs have outplaced inflation for each of the years since World War II are...
Health care and higher education.
Yep.
Look where it all really spiked: around the time of HillaryCare. I guess if you can't "reform" it, you regulate the heck out of it!
Administrators = Government + Lawyers
It's apparently sourced, but first match only finds usage in this Feb 2016 slideshow:
http://www.slideshare.net/athenahealth/thriving-as-an-independent-practice
I can't make sense of it. The vertical axis is a percent, but what scales 100%? It starts with near 0% in 1970. If you look at the 100%, the administrators cross that around 1975, while the doctors cross 100% around 1995. So what could that mean!?
Here's another one, with doctors, nurses, and administators in slide 60, and something similar 1970-1998, starting near zero, and rising over 2000.
http://www.slideshare.net/bayarea/healthcare-presentation-iafpe-sep-12-2009
Okay, so maybe 0% is what I'd call 100%, and 100% is a doubling. So the number of administrators in 1998 is 20 times as many as 1970, while doctors slightly more the doubled, 1.3 times more. And nurses rose more than doctors, which at least makes sense, shifting care tasks to lower skilled workers.
I wouldn't suppose people like lab technicians would be "Administrators", but it makes sense with more diagnostic technology there'd be more non-doctors doing work that didn't exist in 1970. But I'd not assume that meaning.
One more chance on source statement...
Bureau of labor statistics; NCHS; and Hammelstein/Woolhandler analysis of CPS Growth of Administrators 1970-2009
Who are Hammelstein/Woolhandler?
Ah, pro-single payer! So now I wonder if they're also including the insurance industry?
http://www.bostonglobe.com/opinion/2012/06/01/single-payer-health-care-would-save-billions-for-massachusetts/yNTLRlKucgdJCUCU3P5arM/story.html
-------
Here are six alternative steps the Legislature could take that would actually save money while still preserving care.
■ Cut out the middlemen. Why exactly do we pay private insurers 10 cents of every premium dollar? The plan that covers all 13 million residents of the Canadian province of Ontario has overhead of only 1 percent. Adopting that single-payer approach in Massachusetts would save about $2 billion in insurance overhead in 2013 alone.
■ Pay hospitals the way we pay fire departments: real global budgets that cover all operating costs, not the per-patient schemes that are masquerading as global payments. Billing, collections, and paperwork consume nearly one quarter of hospitals’ revenues. Eliminate billing for individual patients and you’d cut that nearly in half. The savings: about $3 billion in 2013.
■ End the medical arms race and enforce real health planning.
■ Right-size the physician work force: more primary care, fewer specialists.
■ Negotiate drug prices statewide. Canadians pay 40 percent less for drugs than we do because they use single-payer buying power to drive down prices from pharmaceutical companies. Why can’t we?
■ Cap health executives’ incomes. Why should a hospital CEO make more than the president of the United States?
David U. Himmelstein, M.D. and Steffie Woolhandler, M.D., M.P.H. co-founded Physicians for a National Health Program. They are professors at the City University School of New York School Public Health and visiting professors at Harvard Medical School. They worked as primary care doctors in Massachusetts from 1982-2010.
------
Ares, if you believe single-payer healthcare works, you'll believe in leprechauns, fairies and yetis, too. Just give me one example where central planning works in the long run. No one person, organization or entity is capable of running 1/7th of the American economy, or much else. None of those six alternative steps will work.
My favorite part is: "Negotiate drug prices statewide." So we'll have 51 different states negotiating drug prices, eh? Well, if 51 is great, why not one? That's what single-payer is: ONE single payer. Canadians pay 40% less for drugs because they're free riders on pharmaceutical innovation. Unless medical innovation isn't important to you, and you're willing to submit to rationed care at the discretion of some nameless, faceless, unaccountable bureaucrat. You probably believe you can have "Better care, at a lower cost." Just like "If you like your doctor, you can keep your doctor."
And please enlighten me about why the President of the United States' annual salary has anything to do with a hospital CEOs compensation package? Do you understand anything about compensation structures?
The government knows all, sees all, and can produce any outcome. That's magical thinking. Central planning never works in the long run... it never lives up to its promises. Quality descends and costs skyrocket. For anything it touches. When will you people ever understand the human condition, and that government is run by human beings? Why would you ever want to centralize human flaws into one source? What is it that scares you so much about distributed sources? I thought we were supposed to "celebrate diversity." The government kills diversity.
Then again, you believe in anthropomorphic climate change. How do you like the states attorneys general going after private companies and think tanks for their dissent? Celebrate diversity, indeed! We'll have all kinds of diversity... just not the thought kind!
The Left claims to be the vanguard of some euphoric free-for-all xanadu society. What we end up with is the misery of totalitarianism.
The truth will set you free.
When you have no argument, you attack the data.
Anonymous at 2:36 PM said... When you have no argument, you attack the data.
Who is attacking and what data?
My small accomplishment was to discover the source the graph was by two doctors supporting single-payer for Massachusetts.
I'm not sure what IAC is ranting about, although lots of bitterness there.
On the 51 plans, Minnesota is also looking at single-payer plans, and once individual states show that works, it makes sense other states won't bother reinventing the wheel. Perhaps it will end up as regional things with groups of like-minded states working together.
Soon I guess Minnesota and Company can also be "free riders on pharmaceutical innovation." It'll be a good deal for us.
Who knows, maybe there are better business plans than "invent a drug, make up a illness that it helps, suppress the side-effects, give free samples to doctors, and complain that the 10,000% markups are just market economics in play."
Anyway, life will be better when some of that "administration" bloat that Stuart discovered is reduced. Or at least maybe we can figure out who they are and what they're doing before we make their jobs obsolete.
I guess I'm a bitter clinger, Ares. I'm bitter about people believing self-evident economic stupidity and I am clinging to as much of a private healthcare system as possible.
Perhaps you could at least consider -- if just for a moment -- that the increase in administration is because there's more to administrate. What's driving the need for so much administration? Did you ever once consider that? What they're doing is keeping government, insurance companies and lawyers at bay... just like education. Government workers, trial lawyers and teachers unions are significant Democrat donor constituencies. How is it you can be so cynical about the private sector's motives and ignore the public sector's motives? Do you really think government will make things FREE?
Democrats celebrate diversity and are pro-choice... unless it's economic diversity or economic choice.
Your level of ignorance is breathtaking. Government will solve all our problems! Enjoy your single-payer plan in Minnesota.
IAC, for some reason public funded roads are okay for you, but public funded health care is not. Do we think roads are free? No, we pay taxes for them, and the rich pay a larger share.
As long as we require hospitals to treat everyone with emergency care, you can be sure some people are not going to have insurance, and not go in until they need emergency care and can't be refused. And hospitals pass on those costs to everyone else.
And if you don't have insurance, and plan to pay with cash you'll face "charge masters" rates that are jacked up many times higher than anyone actually pays who has insurance, because insurance companies can refuse to pay more than some amount, and different insurance companies have different rates they'll pay, so hospital "charge master" rates exist to maximize returns from all the permutations of insurance companies polices in an endless evolutionary war of attrition.
And if you're Ron Paul with $100,000 in your savings account, and no insurance, good luck trying to negotiate which hospital emergency room will give you the best price on your surgery after your car accident. You can refuse to pay of course, and then see your credit score plummet, which actually might not be a bad thing if you have $100k in the bank and no need for credit. I'm not sure all the things debt collectors can do to you, but I'm sure they can make your life miserable if you owe enough.
including responses from January-September 2015. It's a brief history of lack of access to needed medical care in the U.S.: odfmedical.com
Post a Comment